

It’s Birth Trauma Awareness week. Birth trauma means a lot of different things to different people. As I write there is a debate unfolding on Twitter about how birth trauma should be defined. At one pole is the argument that only physical trauma is a legitimate definition, at the other is the argument that birth trauma should be defined by the birthing woman in any way she wishes. I don’t have a definitive position on that argument. As a researcher, I am interested in the way that official birth records represent birthing women and their bodies. This week I thought that it might be interesting to use my analytical skills to look at the most recent Queensland Perinatal Data Collection report (the statistics for 2019) and see how birth trauma is accounted for in an official record.
All hospitals and maternity care providers in Queensland (an Australian mainland state) are legally required to report particular data to the Perinatal Data Collection service. Data from the Perinatal Data Collection are taken very seriously, used to demonstrate improvements (or not) in care over time, and support arguments for how government money is used in maternity care. A committee of people have selected what is, and is not, collected and how the various terms are defined. The list of data required is therefore a socially determined product, and hidden within it are the beliefs, values, and assumptions of the people who have played their part in generating the list since it began. Analysis of the products of their work can provide a glimpse into these beliefs, values, and assumptions that informed the development of the data collection service and its reports.
Searching for the word “trauma” identified six tables. The tables reported labour and birth complications according to mode of birth and provided detailed lists of different types of genital tract trauma, sorted according to whether surgical repair was performed and the professional designation of the accoucher. In total, 59,540 women gave birth in Queensland in 2019, with 38,506 giving birth vaginally (65%). Of the women who gave birth vaginally, 4% (1,608) had a forceps assisted birth and 12% (4,562) had a vacuum assisted birth. 21,918 women (35%) gave birth by lower segment or classical caesarean section.
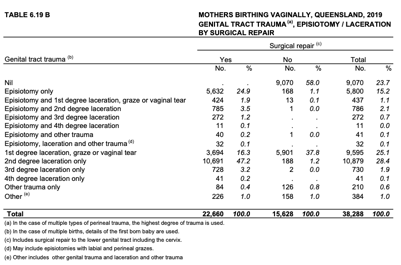
I have chosen table 6.19B for further analysis as it provides the most detail about types of genital tract trauma. A data collection manual set out the definitions that were to be used when clinicians completed the perinatal data collection form. The “nil” option was defined as no damage to the perineum, the category “graze or tear” as a slight abrasion, and the remaining forms of trauma related either to lacerations or surgical incision in the form of episiotomy. Two “other” options sat at the bottom of the table and were not defined in the manual. A summary statement in the manual said:
Perineal laceration (tear) may cause significant maternal morbidity in the postnatal period. Episiotomy is an indicator of management during labour and to some extent intervention rates.
p 60
23.7% of women were represented as having no genital tract trauma. The most commonly assigned category was second degree laceration (28.4% of women). 19.3% of women were reported to have had an episiotomy, 2.7% of women to have damage to the anal sphincter complex (third- and fourth-degree trauma) either in association with an episiotomy or without.
Looking at this data from an analytical perspective, here were the things I noticed. (You might spot others – if you do, please post a comment and share.) First, the only way in which trauma was visible in this official account of what happens to women’s bodies in birth was with respect to physical trauma to the vagina, vulva, and rectum. Any sense of trauma as a form of psychological distress was missing from the data. This focusses organisational efforts on preventing and repairing perineal trauma. It is not particularly surprising then, that programs such as the perineal bundle have been widely introduced in Australia and the United Kingdom, and that debates rage on Twitter about the legitimacy of psychological trauma as a form of birth trauma.
Second, the wording provided in the manual reflects a common belief in maternity care. The statement I quoted above implies that any form of perineal laceration is pathological and likely to result in symptoms after birth. It is also possible to hold the belief that most forms of minor perineal trauma occur as a physiological safety mechanism to permit women to give birth to a bigger baby than will fit through an intact vaginal opening, and they typically heal quickly and well. Episiotomy on the other hand is seen as an indication that the birthing woman has received the active care and consideration of her care provider, and is not seen as an intervention in and of itself (the quote says it only reflects intervention rates). Statements such as this quote both reflect and generate beliefs that spontaneous perineal trauma is bad, but the same degree of trauma electively created by a care provider is good management. It is easy to see how this might drive the use of episiotomy in practice.
Finally, there is a very common form of genital tract trauma that remains absent from the tables. The uterus is part of the genital tract. Caesarean section involves creating an opening large enough for the baby to fit through where there was no natural opening before. This is also a form of surgical trauma, in the same way that episiotomy is, but with more extensive changes to the anatomy. Caesarean section rates are presented in an earlier table, but in this table those women are presumably collected under the “nil” trauma category. The presentation of caesarean section as only a mode of birth and not as a form of genital tract trauma supports the belief that it causes less damage to a woman’s body than vaginal birth. Here we can see how it becomes possible for people to see caesarean section as a way to avoid trauma, rather than a different type of genital tract trauma.
I’m not arguing that we need to change the data collection systems we use and redefine the information we gather in them. But I do believe there is value in being aware that official records such as these were created by particular people, with particular beliefs about birthing women’s bodies, and that these beliefs potentially are expressed once again when we make use of the data contained within. As clinicians, but particularly as researchers and managers, a critical reading of the evidence is vital if we wish to reform, rather than recreate, our maternity care systems.
Categories: Language, Reflections
Tags: Birth trauma, caesarean section, Episiotomy, Perinatal data, Perineal trauma

Beautifully deconstructed. Thank you Kirsten
LikeLiked by 1 person
This brings new insight to our interpretation of the numbers. It also comes at a time when ‘being made to feel guilty’ about caesarean birth has again been raised on social media, without any deeper investigation into those feelings of guilt, their causes, or who is responsible for them.
LikeLiked by 1 person
Thank you for your useful analysis Kirsten. We also need to consider women who suffer back, hip and symphysis pain postnatally, varying degrees of prolapse and incontinence, the side effects of analgesia and anaesthesia etc etc. We don’t collect any real stats on this.
LikeLiked by 2 people
You are correct. Val Slavin has just finished her PhD near me, looking at patient reported outcome measures and has now validated some tools for some of these. Hopefully services will start to pick them up and use them.
LikeLike
Thanks Kristen, an interesting perspective. Reflecting on your comments regarding the woman’s view of trauma. I have recently cared for a woman who had an empowering second birth in the water. As a clinican I was devastated to find that she had a 3rd degree tear, however to her it was very positive which she saw as ‘healing’ from her previous birth experience. Trauma is so individual and how we treat women can impact on their experience of birth.
LikeLike
An important discussion, thank you. I second Mavis Kirkham’s comment on the need to consider postnatal pain, incontinence and prolapse. I am particularly surprised that the latter is not addressed in the data. I thought it important to add to the discussion, though it may be for a different set of data, that whist nipple trauma is not directly from the birth process, the extent of it within 24-48hrs after birth is arguably one of the greatest obstacles for some women in the post natal period and for some individuals more impactful than perineal, Caesarian or emotional insults.
LikeLike
Australians as workers have the same right to protection from psychosocial injury as from physical injury under the Work Health and Safety Act 2009. Employers are compelled to identify psychosocial hazards and put controls in place to reduce psychosocial risks to workers, just as they must with risks of physical injury. Why is this standard not applied to Australians as patients? How can health departments,facilities and professionals not be held as accountable as your average small business owner?
LikeLike
Birthing women are not employees so the laws that protect workers don’t extend to them. There are other ways that health professionals and services are held accountable but they are stacked in favour of the status quo.
LikeLike
As a fellow obstetrician, I found your reflections very interesting. Thank you, for sharing how data is captured. I believe the template used is almost universal. Over the last decade and more, with my growing interest in midwifery-led care and my commitment to promoting midwifery in my country, I have become aware of how poorly we obstetricians understand what women truly want and what birth trauma is all about- sigh! I have shared your article with my fraternity in my place of work.I hope you will send in an abstract for the NLBC virtual conference we are hosting in Dec ( 2nd-3rd) 2020. Would love to hear from you.
LikeLiked by 1 person
Thanks Evita – I remember having a lovely conversation with you on the train platform after the last NLBC. I’ll put some thought into an abstract.
LikeLiked by 1 person
Thank you for our thoughts on this issue. My apologies for not responding to this earlier. I think your statistics are much more comprehensive than those collected in the UK. Having said that, however, there is a glaring hole in both sets of data. Postnatal depression, post-traumatic stress and maternal suicide should also be included.
People have said that PTSD is more common but we have no idea of the numbers. Also, many years ago (around 2000) Jean Robinson and I met with Dr Gwyneth Lewis who was the head of the Confidential Enquiry into Maternal Death in the UK. We explained to her that we were concerned about the numbers of women who committed suicide many years after the birth of their last baby. We urged her to conduct an inquiry up to 5 years after the birth, because so many women hang on for the sake of their children, and invariably suffer in silence. Gwyneth did not have the funding for five years, but she did look into suicides up to one year after the birth and found in 2002 that suicide was the leading cause of maternal death. In 2014-2016 report it had slipped to the second leading cause, but the latest report 2015 to 2017 make no mention of maternal death.
I meet so many women who are traumatised by their birth experiences so looking at PND, PTSD and maternal suicide should be included in birth statistics and any investigation into maternal trauma.
Ref: CEMACH (2004). Confidential Enquiry into Maternal and Child Health, Why Mothers Die 200-2002, Sixth Report, RCOG Press, London.
LikeLiked by 1 person
I don’t have the numbers at hand, but the Qld data has in the past shown that suicide is a significant cause of maternal death in the year after birth. It’s definitely something we need to be measuring in routine data collection.
LikeLiked by 1 person