
(Originally posted in October 2020, this post has been refreshed and updated.)
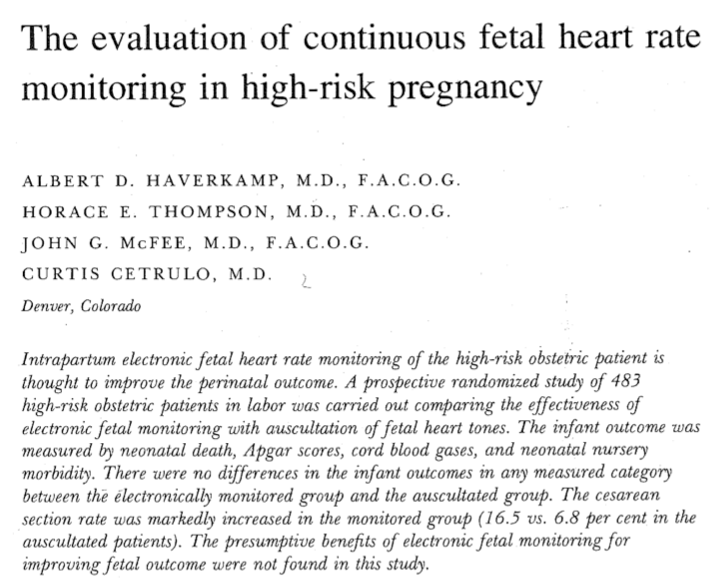
I suspect that when asked to discuss the evidence about CTG monitoring, many maternity professionals would struggle to name a specific paper, and those who did would probably mention the “Dublin trial” (McDonald, et al., 1985). There have been eleven randomised controlled trials which have compared CTG monitoring with intermittent auscultation. The first ever trial was published in 1976 by the Denver, USA based team of Haverkamp, Thompson, McFee, and Cetrulo. When I first read it, I found it fascinating. I’d like to draw it to people’s attention as I think it raises an interesting question which has been essentially ignored in research since then.
Why was the research done?
In 1976, CTG monitoring had been in use for a decade and it was widely assumed to have played an important role in the fall in newborn deaths that had been documented over that time period. As the research team pointed out, leading obstetric authorities of the time were calling for the routine use of CTG monitoring, yet there was no good quality evidence to support this. There were a bunch of before and after type studies, but there were so many other changes happening at the same time (like the introduction of ultrasound and intensive care nurseries) that it was impossible to know what was actually working and what wasn’t. Another research team had previously attempted to obtain ethical approval to conduct a randomised controlled trial, but this had been denied, on the basis that it was unethical to withhold CTG monitoring (Martin, 1998). (The irony of which is now apparent in retrospect!)
What did they do?
483 women considered to be at high risk for poor perinatal outcome were recruited for the trial. A numerical scoring system for risk was used (but the details of this were not given in the paper) to decide who to include. In addition women with meconium stained liquor, who had abnormal heart sounds on auscultation at admission, or when an oxytocin infusion was in use were also approached to take part in the study.
Women were approached in early labour or if they were being induced and ALL those who agreed to take part in the trial had a fetal scalp electrode and an intrauterine pressure catheter inserted. Once this was done, women then were randomised to either intermittent auscultation or CTG monitoring. When randomised to intermittent auscultation, the CTG monitor was moving out of the room, covered, and the CTG trace was not used to guide management during labour. This group of women had the fetal heart rate monitored by a “study nurse” every 15 minutes in the first stage and every 5 minutes in the second stage of labour. Women randomised to CTG monitoring had the monitor in the room, did not have the study nurse listen intermittently, and the CTG trace was used to guide clinical management.
It is this particular design that makes this study so interesting, as it meant that a CTG trace was available to be looked at later, even for the women who had intermittent auscultation. No other trial has used the same approach. Doing the study this way reduced the difference between the “intervention” and the “control” groups as the only difference was the addition of intermittent auscultation in the “control” group. In other trials, only women randomised to CTG monitoring would have the interventions associated with internal monitoring, and differences in outcome (like infection relating to the use of internal monitoring equipment) might have been due to this.
So what did they find?
There were no stillbirths during labour, and three neonatal deaths: two of which occurred in the group monitored by CTG. There were no significant differences in cord blood gas results, low Apgar scores at 1 or 5 minutes, or any other outcome for the baby, including seizures.
There was a statistically significant increase in caesarean section (both for any reason, and specifically for fetal concerns), a higher rate of general anaesthesia, and a higher rate of postnatal infection for women when CTG monitoring was used, which remained the case when corrected for the higher rate of caesarean section.
The authors were surprised
The apparent lack of improvement in outcome in high-risk pregnancies by the use of electronic fetal monitoring in this study in comparison to auscultation is unexpected, when considering the current opinion expressed in the world literature.
Haverkamp, et al,., 1976, p. 316
Buried in the middle of the paper is the bit I found most interesting. There were more “ominous” CTG abnormalities in “early” labour (prior to five cm of cervical dilatation) when intermittent auscultation was not in use and the CTG was being used to guide decisions about labour. Given that everyone had the monitoring equipment attached – this is rather unexpected. The authors had a theory to explain this difference:
The patients who were auscultated had individualized nursing care with one of the project nurses at the bedside almost continually. Very close physical contact with the patient was necessary for the nurse to auscultate the fetal heart tones adequately. This was not true to the same degree with the monitored group. Nursing attention to the gravida with respect to maternal comfort, emotional support, and ‘laying on of hands’ could have a significant impact on the fetus. Also, despite the fact that a monitor was attached to the patient, the machinery was not at the bedside but in the hall. Patients who have a monitor adjacent to their bed are often bothered and stressed by flashing light, the sound produced by each fetal heart beat, and hearing or seeing decelerations even when they are benign. The authors have the impression that the reassuring psychological atmosphere created by personal nurse interaction and the absence of the recording machine in auscultated patients contributed to the excellent infant outcome in auscultated patients.
Haverkamp, et al,., 1976, p. 316
So can CTG monitoring affect the fetal heart rate?
Which leads me to the question that remains unanswered in all subsequent research: could heightened anxiety in the birthing women because of the presence of the CTG monitor and the relative absence of personalised midwifery / nursing support create the very problem that the CTG monitor was designed to address?
There are some clues that back this up as a possibility. Shalev, et al. (1985) found significant increases in the levels of several stress hormones during and for 30 minutes after antenatal CTG monitoring was performed. More recently, Mancuso, et al. (2008) recorded higher levels of anxiety after antenatal CTG monitoring. Higher levels of stress hormones may cause redistribution of blood away from the placenta, decreasing fetal oxygen levels and therefore initiating compensatory fetal heart pattern changes (Buckley, 2015).
What fascinates me the most about this unanswered, yet really important question is that in the 49 years since this paper was published, no research group has followed up on this. There are certain areas of that attract the interests of obstetric researchers and the organisations that fund them, and others that are simply ignored as they don’t support the big story that CTGs are useful. This is obviously one of those. I wonder if we will ever find the answer.
Sign Up for the BirthSmallTalk Newsletter and Stay Informed!
Want to stay up-to-date with the latest research and course offers? Our monthly newsletter is here to keep you in the loop.
By subscribing to the newsletter, you’ll gain exclusive access to:
- Exciting Announcements: Be the first to know about upcoming courses. Stay ahead of the curve and grab your spot before anyone else!
- Exclusive Offers and Discounts: As a valued subscriber, you’ll receive special discounts and offers on courses. Don’t miss the chance to save money while investing in your knowledge development.
Join the growing community of BirthSmallTalk folks by signing up for the newsletter today!
Sign up to the Newsletter

References
Buckley, S. J. (2015). Hormonal physiology of childbearing: Evidence and implications for women, babies, and maternity care. https://www.nationalpartnership.org/our-work/resources/health-care/maternity/hormonal-physiology-of-childbearing.pdf
Haverkamp, A. D., Thompson, H. E., McFee, J. G., & Cetrulo, C. (1976). The evaluation of continuous fetal heart rate monitoring in high-risk pregnancy. American Journal of Obstetrics and Gynecology, 125(3), 310-320.
Mancuso, A., Vivo, A., Fanara, G., Denaro, A., Laganà, D., Accardo, F. (2008). Effects of antepartum electronic fetal monitoring on maternal emotional state. Acta Obstetricia et Gynecologica Scandinavica, 87(2), 184 – 189. https://dx.doi.org/10.1080/00016340701823892
Martin, C. (1998). Electronic fetal monitoring: a brief summary of its development, problems and prospects. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 78(2), 133 – 140.
MacDonald, D., Grant, A., Sheridan-Pereira, M., Boylan, P., Chalmers, I. (1985). The Dublin randomized controlled trial of intrapartum fetal heart rate monitoring. American Journal of Obstetrics and Gynecology, 152(5), 524-539. https://dx.doi.org/10.1016/0002-9378(85)90619-2
Shalev, E., Eran, A., Harpaz-kerpel, S., Zuckerman, H. (1985). Psychogenic Stress in Women During Fetal Monitoring (Hormonal Profile). Acta Obstetricia et Gynecologica Scandinavica, 64(5), 417 – 420. https://dx.doi.org/10.3109/00016348509155159
Categories: CTG, EFM, History, IA, Perinatal mortality
9 replies ›
Trackbacks
- Risks of CTG monitoring: Part 3 – Birth Small Talk
- Does CTG monitoring during labour work? – Birth Small Talk

Thanks for bringing this early paper to our attention Kirstan. Brilliant.
LikeLiked by 1 person
You are welcome Teresa. I always find older research fascinating!
LikeLike
This is such good evidence even when monitoring when CTGS volumes are turned right down and not the focus with cordless -off the bed and ability to be distracted eg in the shower, music low lite rooms. Of course midwifery presence with respectful distances can be added positive and safe feelings for the woman.
LikeLike
I think that quiet and calm presence is so important. The midwife’s autonomic nervous system is balanced, and that helps balance the woman’s, and that helps balance the baby’s heart rate too. And probably reduces oxygen requirements at the same time.
LikeLike
What an interasting paper! Yes, from all we know now it is true that relationship with and companionship of a midwife improves outcomes and experience.
This is what I see as a threat of antenatal and intrapartum routine use of CTG, the stress, which is not at all adressed… I wonder if UltraSound has also this effect?
In Poland many women have antenatal CTG, many have it continous, even if wireless, and US is performed often at every antenatal visit 😦
LikeLike
*continous – I mean during labor
LikeLike
I have never taken a deep dive into the effect of ultrasound on the fetus but it is my impression that it has been under researched compared to the amount of exposure some fetuses now have.
LikeLiked by 1 person